
A quick summary of the clinical processes that go into diagnosing a stroke and the general forms of treatment offered.
What is a stroke?
A stroke is a type of medical emergency that occurs when blood supply to the brain gets interrupted due to some reason. Worldwide, it is the second leading cause of death and the third leading cause of disability [1]. The property that makes strokes so deadly is the amount of time the patient has, to get treatment before the problem advances to a serious stage. Since cells in the brain require a constant supply of blood, even the smallest of delays can lead to the death of brain cells, most of which can not be regenerated. Typically, patients have a great chance of full recovery if they get treatment hours of the first symptoms. Even in the best scenarios, there can be some irreversible damage to the brain.
Strokes or cerebrovascular accidents are primarily due to either of 2 reasons; Ischemia or Haemorrhage.
Ischemic:
Ischemic strokes are caused when a blood vessel gets blocked off due to some kind of obstruction in it. This is usually due to plaque buildup in the blood, or a clot in the bloodstream. Transient Ischemic Attacks (ministrokes) is a type of stroke that happens due to Ischemia in the brain arteries but they usually clear up on their own after some time, hence lasting only for a short period.
Haemorrhagic:
Haemorrhagic strokes happen when a blood artery ruptures and begins leaking blood inside the brain. As a result, blood does not reach where it was supposed to, and some parts of the brain are deprived of Oxygen and nutrients. These strokes are usually more deadly as compares to Ischemic strokes as the increased blood volume inside the brain applies pressure to the rest of the brain and results in more damage.
How does one recognise a stroke?
To recognise stroke symptoms, the general heuristic is to look at the Face, Arms, and Speech of a person. An easy way to remember this is to remember the acronym FAST.
- Face: If the patient’s face is drooping on any side
- Arms: If an arm is more difficult to move than the other.
- Speech: If there is slurred speech
- Time: If any of the above is true, its time to call the ambulance as these are signs of a stroke.
The symptoms mentioned above happen when the part of the brain controlling them starts becoming deprived of oxygen.
Diagnosis

Image authors: here
From symptom detection to the hospital ER
Once the symptoms are detected, the patient is rushed to the hospital. The patient is taken to an emergency room and rushed for imaging after drawing blood [2]. If the patient is conscious and the symptoms are mild, then physical examination is done by a neurologist to better determine where to look for the bleed in imaging [3]. Other risk factors such as existing conditions are also considered. These include but are not limited to Hypertension, Cholesterol, smoking habits, and heart conditions. Basically, any condition that may affect the blood pressure (as high blood pressure is often the cause of haemorrhages).
Blood tests are also done parallelly to determine if the cause of weakness / unconsciousness is due to low haemoglobin [4]. The Complete Blood Count (CBC) is used to check for blood conditions. These may also help determine the Etiology of the stroke (i.e cause of the stroke). For example, if the platelet count is low, then there is a higher chance of it being a haemorrhagic stroke. Electrolytes and Blood Sugar imbalance may also cause stroke-like symptoms. For eg., a low amount of Sodium in the blood can cause impaired electrical activity in the brain, which gives the same symptoms as a stroke. Similarly, Hypoglycemia or low blood sugar can also cause stroke-like symptoms. There are certain proteins in the blood that can cause excessive coagulation, this is checked for as well. Finally, a toxicology report is also created to check for substances which mimic stroke symptoms [5].
Imaging
Imaging is one of the important confirmation tests done when a stroke is suspected. This is where the etiology of the stroke is determined. Primarily, there are 3 ways in which the brain can be imaged.
CT scan: The fastest method is a simple head CT scan as shown below. While the resolution of this image is less, haemorrhagic strokes can be easily identified in this scan as blood is visible as bright white (since it is denser than the surrounding tissue) on this scan. Any area that should not have blood, but is showing up white on the scan can immediately be identified as an area of haemorrhage. Ischemic strokes are not that easy to identify with just a simple CT scan as the areas deprived of blood can seem just as dense as the other regions for quite a long time. After some time, however, the deprived region starts to appear darker in the CT scan as the cells keep dying. In a CT scan, the amount of white color in a spot is proportional to its density. Dense spots show up as white, light spots show up as black/grey.
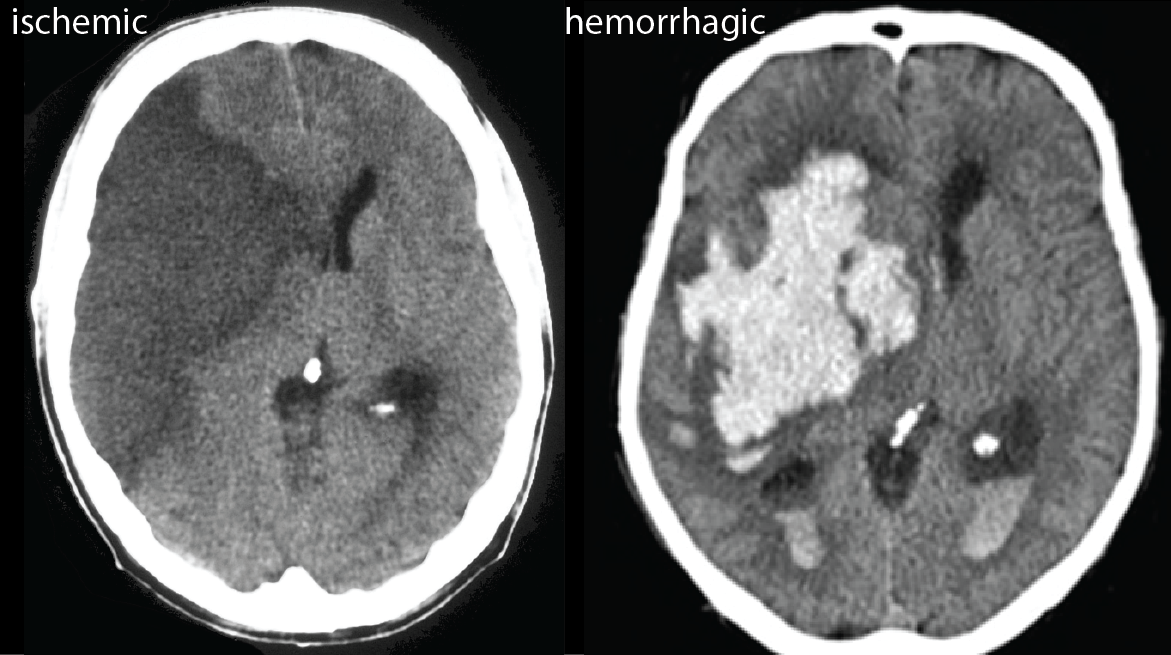
(left) CT of an ischemic stroke. Left side of the image is dark, showing that the density of parenchyma there has decreased due to dead cells. In general, it takes time to detect ischemic stroke as the difference in density is not very apparent in early stages of the stroke. (right) CT of a haemorrhagic stroke. the bright pool of blood visible on the left is a haemorrhage. Image authors: here
CT Angiogram: For ischemic stroke detection, a CT angiogram is created to picture the blood vessels in the brain. This is a normal CT scan, but the patient’s bloodstream is injected with a fluid that lights up on the CT images. These images are then cleared off of any tissue, and only the vessels are highlighted. This can show if an artery has a sudden breaking off point, which may indicate a blockage.
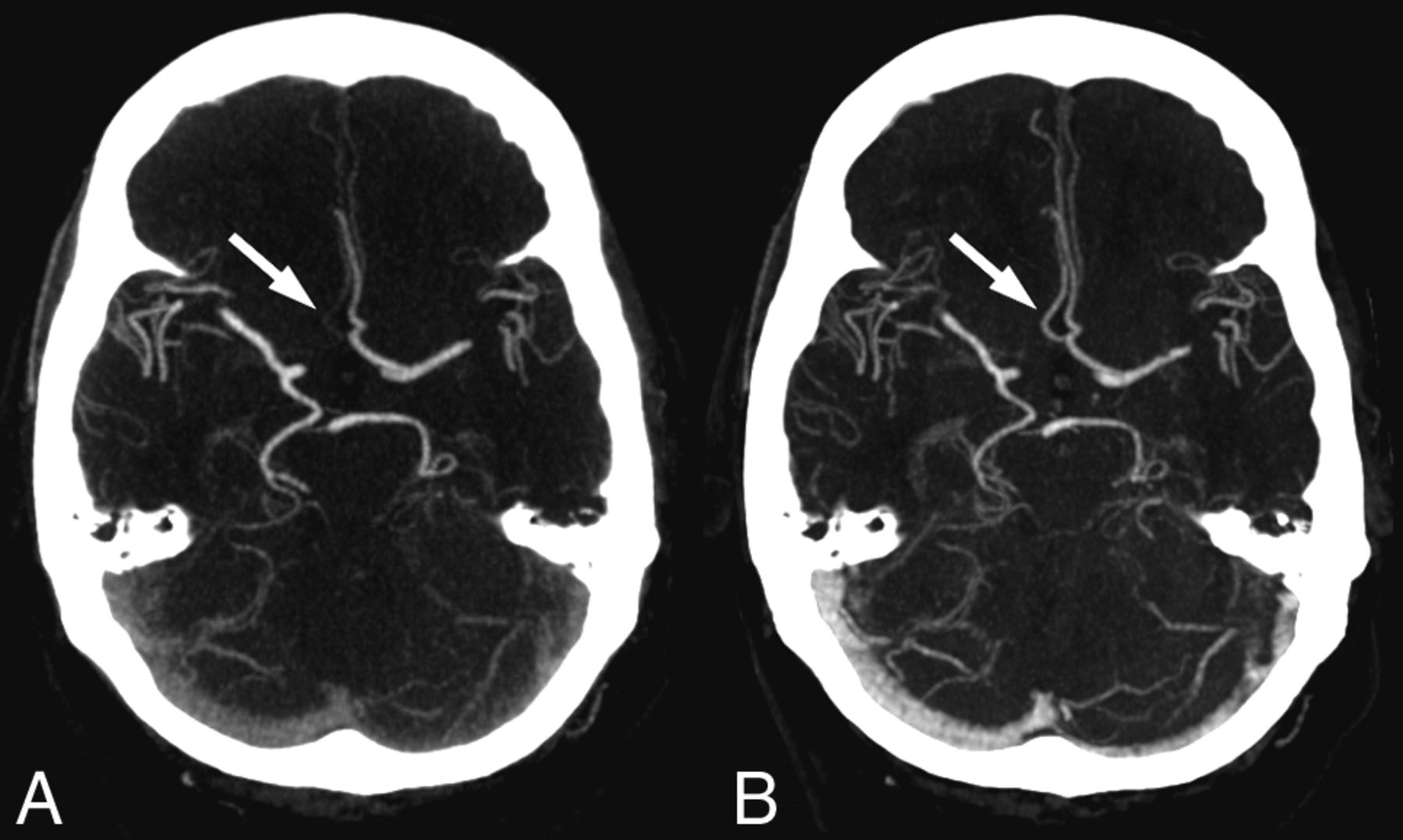
Typical CT angriogram. In image A, you can see one of the vessels splits into 2, but one of the splits is not as bright as the other. This indicates some kind of blockage. The gradient of density change is also very sudden at that spot. You may also notice that the folds of the brain, and other tissues are not visible in this image. Image authors: here
MRI Scan: Finally, an MRI scan shows tissues of the brain in very high resolution. While this scan is expensive and takes quite a bit of time, it provides a very high-quality image, from which blood circulation can be judged easily. CT scans are recommended to be performed if the patient is present in the ER within 6 hours of symptoms [6], whereas MRI scans are preferred for post-treatment uses.
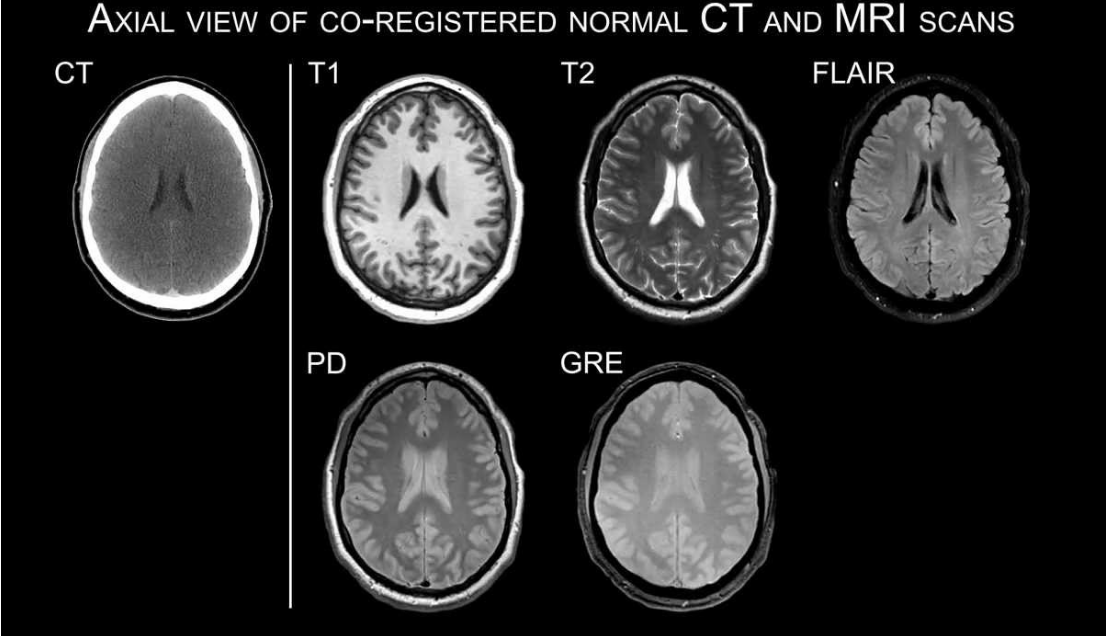
CT scan on the left as compared to different kinds of MRI on the right. Notice how basically none of the brain folds are visible on the CT while in the MRI, most tissues are distinguishable. Image authors: here
Treatment
Ischemic
Thrombolytics: These are drugs that are targeted to destroy blood clots (thrombus) in the bloodstream. For Ischemic strokes, these are often the first choice of treatment and require no further work to destroy the clot. However, these are only effective if administered quickly after symptoms present themselves. A window of 4.5 hours is defined by the National Institutes of Health, USA [6]. The most commonly administered thrombolytic is called Tissue Plasminogen Activator (tPA) [7]. Aspirin generally follows thrombolytic therapy, as it is an anticoagulant, and helps in keeping the blood from clotting again.
Here, you can appreciate why knowing the etiology of the stroke is very important. If an anticoagulant or thrombolytic is administered in a haemorrhagic stroke case, that will make the situation much worse as the ruptured artery would not be able to stop bleeding through clotting!
Endovascular treatment: In cases where the clot or blockage has become too big for drugs to work effectively, a mechanical operation is performed to remove the clot from the blood vessels. These can be of various types/forms. Some well-known methods are mentioned here:
- MERCI Retriever: This is a sheathed wire that is inserted into the blood vessel. Usually inserted through a completely different area (eg. through groin arteries), it is eventually brought to the blocked vessel. The wire is pushed in from behind and brought in front of the clot. Then sheath is pulled back so that the end of the wire is revealed. The wire itself tends to coil, hence forming a net to catch the clot. The wire is now pulled out and it brings the clot out with it. This method was the first of its kind mechanical procedure to be approved by the FDA.
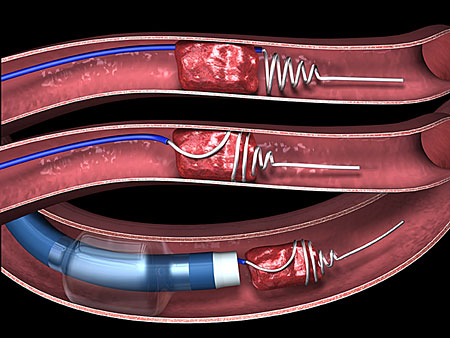
Image authors: here
- Aspiration catheter: This is a suction-based method. A tube is inserted into the vessel and brought near the clot. The clot is then poked with a wire while the tube sucks in all the plaque.
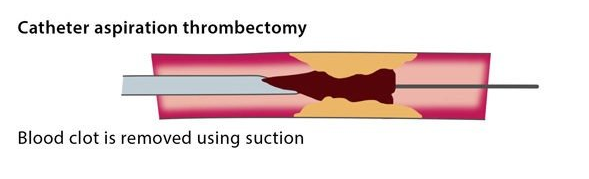
Image authors: here
- Stents: This wire is used to push the cloth to the periphery of the vessel, allowing blood to flow from the middle and clean up all the pieces.
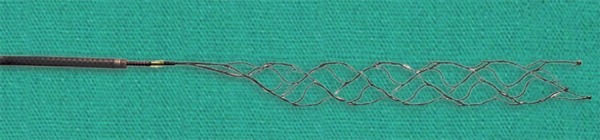
Image authors: here
Haemorrhagic
Intra-cranial Pressure management: While this is not a solution to the problem, this is one of the most important parts of the treatment. The greatest risk in a haemorrhagic patient is damage to the brain due to increased intracranial pressure. The intracranial pressure is recommended to be kept below 20mm Hg [8]. While general medication is administered to keep this low, there are mechanical methods to do this as well. Some of these are mentioned below:
-
Ventricular drains: Ventricles are cavities in the brain which produces Cerebro Spinal Fluid (CSF) which is an important fluid for the nervous system. Drains are attached to these areas because, during a haemorrhage, blood starts filling up these cavities. Drugs are also used to separate blood from the CSF.
-
Blurr hole: If necessary, a surgeon will cut the skull bone (with a small drilled hole called a “burr hole”) to decrease the compression of the brain tissue.
General Medication: Unlike in Ischemic strokes, there is no common drug-based treatment of haemorrhagic strokes. So, medication only caters to manage the patient before surgery can be performed [8].
-
Anti-hypertensive: Due to a rupture in the artery, the heart tries to pump more blood to get it to reach the brain, which increases the blood pressure. This can increase the pressure inside the skull, which can cause a lot of complications as mentioned earlier. Therefore, these drugs are administered to prevent very high blood pressure. Moreover, ventricular drains are attached to the back of the patient to keep the pressure low.
-
Homeostatic Therapy: This is given to counter the effects of any older medication, eg. Aspirin/Warfarin (which are anti-coagulating in nature, and might prevent the rupture from naturally healing).
-
Anti-convulsive: When blood leaks into the brain, the pressure it exerts can cause problems with the normal electrical signals inside, and end up causing seizures. These drugs are administered to prevent seizures from occurring.
Mechanical procedures: There are many mechanical ways of treating haemorrhagic strokes.
- Clipping: For haemorrhages caused due to bursting of aneurysms (a ballooned area of the vessel which is weakened). Clipping is a surgical method where, the base of the aneurysm is shut using a clip, so the blood stops flowing in that direction.
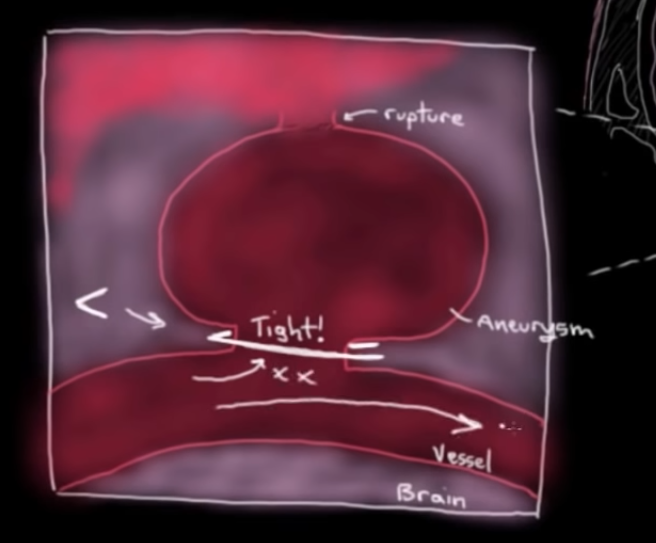
Image authors: here
- Coil embolization: The aneurysm can also be blocked off using a special wire. This is a wire similar to that used in the MERCI retriever. It is placed inside the aneurysm and then its sheath is removed. It is allowed to keep coiling inside the aneurysm till the entire bubble is filled with the coil, moreover, blood clots form on this coil, making a tight seal, allowing normal circulation of blood to the brain.
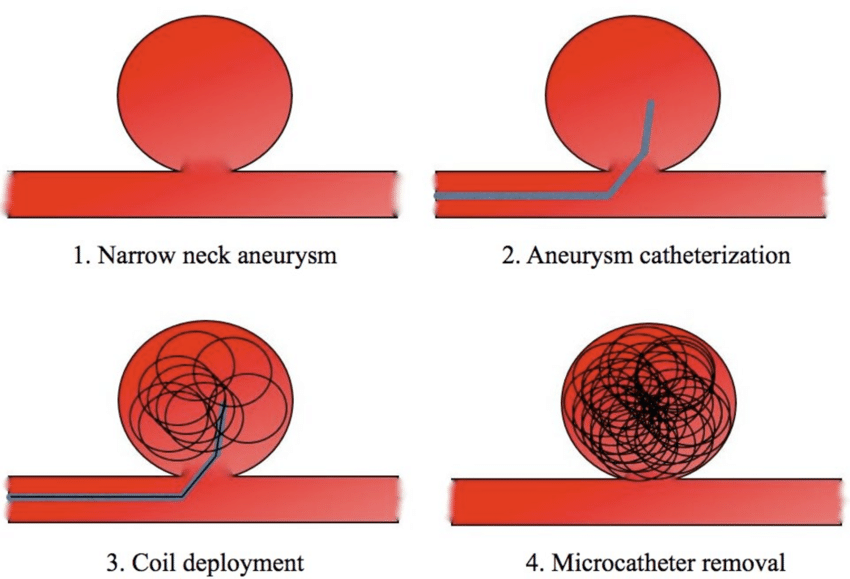
Image authors: here
The most important thing about stroke treatment is the time between symptoms and treatment. Here is a graph showing the chances of survival with amount of delay in treatment. This picture is from a UCLA presentation available online. The title of this slide was Time is brain
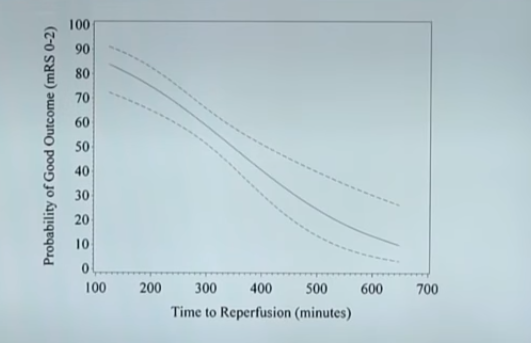
Image authors: here
BIBLIOGRAPHY
Video sources
- Khan academy’s series on stroke:
- UCLA Interventional Radiology : here
Other sources
- WHO report on stroke statistics: here
- Typical issues with stroke treatment (literature survey) : here
- Article on patient workflow optimization: here
- Acute Ischemic stroke guidlelnes by NIH: here
- Intracranial Haemorrhage management by NIH: here
If you want to hear nice music by The Strokes instead, go here