
A quick summary of the clinical processes that go into diagnosing a traumatic brain injury and the general forms of treatment offered.
What is a traumatic brain injury?
Traumatic brain injury (TBI) is a form of acquired brain injury. It occurs when a sudden trauma causes damage to the brain. TBI can result when the head suddenly and violently hits an object, or when an object pierces the skull and enters brain tissue [1]. Typically a result of road accidents, sports injuries, or assaults. The impact that causes the head to jerk suddenly causes a primary injury. Symptoms of this can include confusion, dizziness, or loss of consciousness completely. This is not the end of the story, however. Due to the effects of the impact, certain secondary injuries can appear. eg. A traumatic injury to the head may cause the brain to shift to one side, causing a blockage in an artery, which can cause brain cells to slowly die due to hypoxia (lack of oxygen) in that region.
Depending on the effect of the injury, it can be a focal if it is localised in only one area of the brain or diffused if it is more spread out all over the brain. According to the severity of the injury, TBIs are classified as:
- Mild: the person is awake; eyes open. Symptoms can include confusion, disorientation, memory loss, headache, and brief loss of consciousness.
- Moderate: the person is lethargic; eyes open to stimulation. Loss of consciousness lasting 20 minutes to 6 hours. Some brain swelling or bleeding causing sleepiness, but still arousable.
- Severe: the person is unconscious; eyes do not open, even with stimulation. Loss of consciousness lasting more than 6 hours.
Primary brain injury
When the head is injured, the immediate effect felt due to the mechanism of injury is called the Primary injury. These can be the following:
-
Concussion: A mild injury to the brain. These can occur when the brain shifts rapidly and comes in contact with the skull but no profuse bleeding occurs. Can cause loss of consciousness. Typically heals without any permanent damage.
-
Contusion: This is the bruising of brain tissue. When examined under a microscope, cerebral contusions are comparable to bruises in other parts of the body. They consist of areas of injured or swollen brain mixed with blood that has leaked from arteries, veins, or capillaries.
-
Hematomas: These are blood clots within the brain [called Intracerebral], between the brain’s arachnoid mater (middle lining) and its dura mater (outermost lining) [called subdural] or between its dura and the skull [called epidural]. These clots form due to some form of arterial bleeding. While small clots can be re-absorbed by the brain [2], large ones apply pressure inside the brain and need to be surgically removed.
-
Haemorrhages: These represent more active bleeding scenarios where the blood does not clot that easily, usually due to the rupturing of an artery as opposed to a capillary or vein in hematomas. These can be either inside the brain tissue (Intracerebral) or inside the subarachnoid space (Subarachnoid) which is the space between the innermost lining of the brain (pia mater) and middle lining of the brain (arachnoid mater).
-
Diffuse injury: Injuries that produce microscopic changes that do not appear on CT scans and are scattered throughout the brain. A special type of this injury is called the Diffuse axonal injury (DAI), which occurs due to shearing and stretching of the nerve cells at the cellular level. Axons are a part of the nerve cell which help in communication between cells. DAI can impair this ability to communicate between cells and severely impair the patient.
Secondary brain injury
Continuation of damage to the brain as a result of physiological effects of primary injury is called the secondary injury. This can take from hours to days to occur. Most of the focus during the treatment of a TBI is to control the secondary injuries by balancing a variety of variables such as pressure, oxygen supply to the brain, preventing blockages, etc. [3]. There are a multitude of secondary brain injuries that can occur. The main factors that affect secondary injury are:
-
Cerebral Profusion Pressure (CPP): This is the difference in pressure of the artery (Mean arterial pressure (MAP)) and the pressure already existing in the brain (Intracranial pressure (ICP)). The CPP dictates the amount of blood that goes into the brain, also called Cerebral Blood Flow (CBF). Now, the brain has a fixed amount of space. This includes 80% of brain tissue, 10% of blood, and 10% of CSF (stated in the famous Monro-Kellie doctrine). During a bleed, blood inside the skull can increase, and since the volume is fixed, the pressure inside it increases as well. The body does have regulatory methods to handle this by draining CSF elsewhere, but this can only work to some extent. After that, the ICP starts rapidly increasing, which can cause other parts of the brain to get crushed or damaged. Another effect of ICP increasing is lower CPP and therefore lower CBF. And with lower blood flow, cells can start dying after some time. Here is a graph that explains this effect:
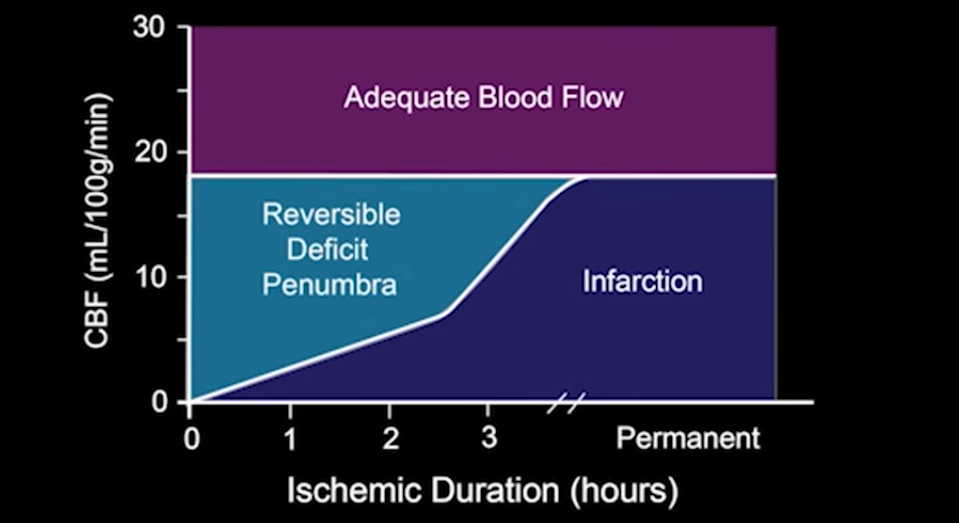
Graph showing the amount of time before cell death begins due to Ischemia (shortage of oxygen). You can see that if the brain gets a CBF of about 18 mL/100g/min for 4 hours, Infarction (or cell death) can begin. With a decrease in CBF, this cell death becomes even faster. Image authors: here
-
Depolarization of axons: The primary injury can cause localized regions of ischemia, which can cause depolarization of neurons in that area [4]. Which leads to loss of potassium ions from the cells. This can ultimately lead to the absorption of water into these cells and cause edema (or cell swelling). Furthermore, this lack of oxygen can also start anaerobic respiration cycles in the cells, which makes a byproduct of lactic acid. Since blood flow is less, this lactic acid also starts piling up.
-
Other external factors: Factors such as blood pressure, metabolic demand of the body, body glucose content, anemia, and electrolytic content in the blood affect cell death in the brain through various pathways. Going into such details would be too in-depth for this overview.
Diagnosis
Preliminary tests
When the patient first arrives. Blood pressure is assessed. Pupils are checked. If the intracranial pressure (ICP) is high, one or both pupils may be very wide. Brainstem reflexes including gag and corneal (blink) may also be tested [3]
The Glasgow Coma Score (GCS) is assessed. It is a 15-point test used to grade a patient’s level of consciousness. Doctors assess the patient’s ability to 1) open his or her eyes, 2) ability to respond appropriately to orientation questions, (“What is your name? What is the date today?”), and 3) ability to follow commands (“Hold up two fingers, or give a thumbs up”). If unconscious or unable to follow commands, his or her response to painful stimulation is checked. A number is taken from each category and added together to get the total GCS score. The score ranges from 3 to 15 and helps doctors classify an injury as mild, moderate, or severe. Mild TBI has a score of 13-15. Moderate TBI has a score of 9-12, and severe TBI has a score of 8 and below.
Imaging
Diagnostic imaging tests are done in the same way as they are done for Strokes. That is, CT scans, CT angiograms, and MRI images are taken. Refer to my post on stroke treatment for an overview of these.
Since most TBIs include a fracture, CT scans are an excellent test of diagnosis. Magnetic resonance imaging (MRI) is not commonly used for acute head injury since it takes longer to perform an MRI than a CT. Because it is difficult to transport an acutely-injured patient from the emergency room to an MRI scanner, the use of MRI is impractical. However, once a patient is stabilized, MRI may demonstrate the existence of lesions that were not detected on the CT scan. [3]
Treatment
Surgical treatment
Emergency surgery is often required to decompress the injured brain and minimise damage. The following are surgical treatments done on the brain to either fix the injury or allow diagnosis and further treatment.
-
Craniotomy: Surgery to remove the haematoma and thus reduce pressure on brain tissue. This involves cutting a hole in the skull to remove a bone flap so that the surgeon can access the brain. The surgeon then repairs the damage (e.g., skull fracture, bleeding vessel, remove large blood clots). The bone flap is replaced in its normal position and secured to the skull with plates and screws.
-
Decompressive craniectomy: This involves removing a large section of bone so that the brain can swell and expand. This is typically performed when extremely high intracranial pressure becomes life-threatening. At that time the patient is taken to the operating room where a large portion of the skull is removed to give the brain more room to swell. The bone flap is stored in a freezer. One to 3 months after the swelling has resolved and the patient has stabilized from the injury, the bone flap is replaced in another surgery, called cranioplasty.
-
Intracranial pressure (ICP) monitor: A catheter is placed through a small hole in the skull and positioned inside the ventricle (a fluid-filled area deep within the brain) to measure the pressure inside the head (figure below). The ICP monitor allows the surgery team to intervene quickly if the pressure becomes too high. Typical intracranial pressure is less than 20 mmHg. However, there are times when a higher number is safe and acceptable.
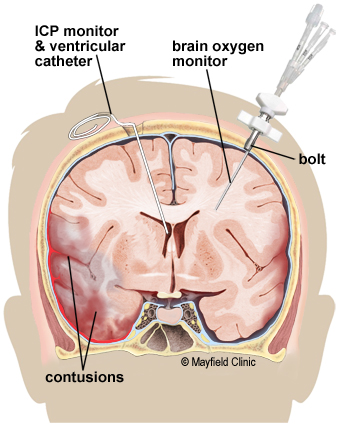
A brain oxygen and cerebral blood flow monitor is inserted into the brain tissue and secured to the skull with a bolt. A catheter is inserted into the ventricle of the brain to monitor intracranial pressure (ICP). If pressure is too high, the CSF fluid can be drained from the ventricles. Image authors: here
-
Brain oxygen monitor (Licox): A catheter is placed through a small hole in the skull and positioned within the brain tissue. The Licox measures the oxygen level and temperature within the brain. Adjustments in the amount of oxygen given to the patient are often made to maximize the brain’s oxygen level.
Medical treatment
Medications can help treat symptoms of TBI and lower the risk of some conditions associated with it. These may primarily include:
-
Coma-inducing medication: This may be given, as a brain in a coma requires far less oxygen. This is therapeutic where oxygen and nutrient supply to the brain is restricted by compressed blood vessels and increased cerebral pressure.
-
Diuretics: Medications designed to increase the amount of water and salt expelled from the body as urine. Given intravenously, can be used to reduce the amount of fluid in soft tissues and thus help reduce pressure on the brain.
-
Anti-coagulants: To prevent blood clots. This is particularly useful in avoiding blockage formation after certain deformations in the brain happen.
-
Anti-convulsives: The large amount of blood in the brain can interfere with the electrical activity and cause seizures and further damage. These medicines are given to prevent seizure-like events.
REFERENCES
Video sources
- ICU Advantage channel’s videos on TBI:
- Overview video by a peditrician: here